
Page 10 - 20230530_vp_02_D
P. 10
vascular professional | issue 02 · 2022
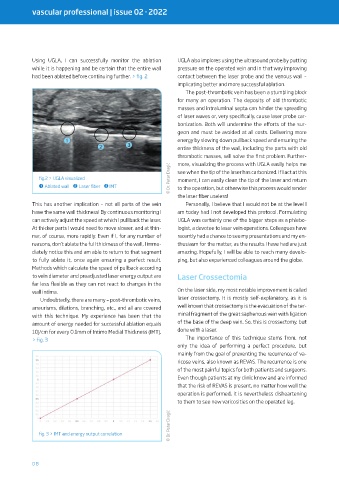
Using UGLA, I can successfully monitor the ablation UGLA also implores using the ultrasound probe by putting
while it is happening and be certain that the entire wall pressure on the operated vein and in that way improving
had been ablated before continuing further. > fig. 2 contact between the laser probe and the venous wall –
implicating better and more successful ablation.
The post-thrombotic vein has been a stumbling block
for many an operation. The deposits of old thrombotic
masses and intraluminal septa can hinder the spreading
of laser waves or, very specifically, cause laser probe car-
bonization. Both will undermine the efforts of the sur-
geon and must be avoided at all costs. Delivering more
➊ energy by slowing down pullback speed and ensuring the
➋ ➌ entire thickness of the wall, including the parts with old
thrombotic masses, will solve the first problem. Further-
more, visualizing the process with UGLA easily helps me
© Dr. Petar Dragić moment, I can easily clean the tip of the laser and return
fig.2 > UGLA visualized see when the tip of the laser has carbonized. If I act at this
➊ Ablated wall ➋ Laser fiber ➌ IMT to the operation, but otherwise this process would render
the laser fiber useless!
This has another implication – not all parts of the vein Personally, I believe that I would not be at the level I
have the same wall thickness! By continuous monitoring I am today had I not developed this protocol. Formulating
can actively adjust the speed at which I pull back the laser. UGLA was certainly one of the bigger steps as a phlebo-
At thicker parts I would need to move slower, and at thin- logist, a devotee to laser vein operations. Colleagues have
ner, of course, more rapidly. Even if I, for any number of recently had a chance to see my presentations and my en-
reasons, don’t ablate the full thickness of the wall, I imme- thusiasm for the matter, as the results I have had are just
diately notice this and am able to return to that segment amazing. Hopefully, I will be able to reach many develo-
to fully ablate it, once again ensuring a perfect result. ping, but also experienced colleagues around the globe.
Methods which calculate the speed of pullback according
to vein diameter and preadjusted laser energy output are Laser Crossectomia
far less flexible as they can not react to changes in the
wall intima. On the laser side, my most notable improvement is called
Undoubtedly, there are many – post-thrombotic veins, laser crossectomy. It is mostly self-explanatory, as it is
aneurisms, dilations, branching, etc., and all are covered well known that crossectomy is the evacuation of the ter-
with this technique. My experience has been that the minal fragment of the great saphenous vein with ligation
amount of energy needed for successful ablation equals of the base of the deep vein. So, this is crossectomy, but
10J/cm for every 0.1mm of Intimo Medial Thickness (IMT). done with a laser.
> fig. 3 The importance of this technique stems from, not
only the idea of performing a perfect procedure, but
mainly from the goal of preventing the recurrence of va-
ricose veins, also known as REVAS. The recurrence is one
of the most painful topics for both patients and surgeons.
Even though patients at my clinic know and are informed
that the risk of REVAS is present, no matter how well the
operation is performed, it is nevertheless disheartening
to them to see new varicosities on the operated leg.
© Dr. Petar Dragić
fig. 3 > IMT and energy output correlation
08